
Children in Nepal: Are they getting quality treatment?

Photo credit: Aastha Ghimire
My grandmother usually shares her story, “We used to fear what if the child doesn’t live longer, so we bore more kids. Maybe I’d have more than just 6 kids had your grandpa not passed away soon.”
Approximately 26 infants out of 1000 died in 2019, which is an improvement following from 216 deaths in 1960. This in itself attests the improvement in Nepal child health care, though the data fails to address urban population(21%), and rural population(79%). Looking at the fertility rate per woman(the chart is modified into per thousand women), women on average gave birth to 6 kids in 1960, but that has reduced to 2 kids in 2019. Socio-economic elements like women empowerment, less discrimination between the son and the daughter, inflation in daily-life cost, and easy access to contraceptive devices mainly rendered this recession. Supposedly, the fear that my grandmother had also doesn’t exist any more due to modern pediatric care.
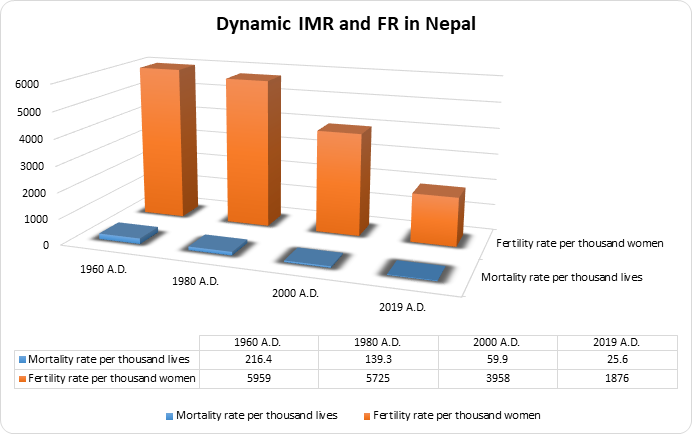
Figure 2: IMR and FR in Nepal.
Data source:The World Bank
Chart prepared by : Aastha Ghimire
“Every child shall have the right to obtain free basic health service” the Constitution of Nepal states this under the right to nutrition and health of children’s rights. With stately promises of health care, almost all private, and government hospitals in the country have a pediatric department, and a few with psychiatric facilities. But the indignation arises in Nepalese when family income solely decides if the child qualifies for the timely treatment or not. Province 6 and province 7, also the economically backward regions of the country, are shown to have the highest childhood mortality, and these particular regions are forlorned initially during micronutrient powder distribution to children, availability of amoxicillin antibiotic, and routine practices for sick children before consultation.
Additionally, a significant positive linear relationship was also shown between district income and the days per month that a few vaccines were provided at facilities. This was true for the Japanese Encephalitis vaccine (p-value: 0.0000005), the BCG vaccine (p-value: 0.0000455), and the PCV vaccine (p-value: 0.0102). Yes, there has been substantial decrease in the respective diseases, however, the districts with low-income receive the immunization fewer days each month. If in future the disease starts spreading again, the concentration hub is likely to be the lower income districts.
After looking at the district level facilities, the paper overviews health facilities in countries like Switzerland, Denmark, Sweden, Thailand, etc. Denmark has the shortest time duration in hospitals out of all EU countries. Medical professionals, pharmacists, doctors and nurses are experts in online procedures, making the online system very strong with data storing. Switzerland, the country with an 8.54 million total population has 985 primary care pediatricians and 5945 general practitioners (caring for an estimated 10%-15% children and adolescents of their patients) in the private for-profit primary care sector. Every Thai citizen is granted universal health coverage throughout all of their lives in Thailand. Coverage by the government has increased access to high-grade medical technology that includes cancer treatments and stem-cell replacements.
On the contrary, child health care is quite expensive for an average income family in Nepal. With a 28.61 million total population, there are around 520 practising pediatricians in Nepal, divesting kids from ample time from the caregiver. This gap between the demand and supply is one major concern of child health care. Also, health insurance facilities are not very popular and the family itself bears the cost of all the treatments. People who come from low income backgrounds are not able to afford the services they require; they tend to withdraw the care or shift to government hospitals. In most cases of premature birth people are not able to afford the services from NICU, which costs 5000 Nepali rupees per day on average.

Figure 3: This picture tries to reveal that health care in Nepal is directly proportional to the family income, and no help from the government side is received.
Photo by: Aastha Ghimire
Adolescent mental health treatment in Nepal has been improving in the last decade. Quoting Dr.Pawan Sharma, a psychiatrist at Patan Academy of Health Sciences, also one of the interviewees :
“Medicines prescribed in Nepal avail worldwide, and follow UK guidelines, and there has been no case of deprivation of medicine”.
What is important to consider is that mental health treatment is centered only in the major cities of the nation making it hectic for people in rural areas to constantly follow-up the treatment. Only one specialized children and adolescent psychiatric hospital, i.e. Kanti Children Hospital is established in Nepal. All other hospitals practise adolescent mental health care under adult care. Biofeedback therapy which was found in international practices is not practised in Nepal, rather psychoeducation is approached. As a low-income country, the latter step looks feasible in the context of Nepal as of now.
The status quo of the mentioned problems are not to be dreaded upon, instead collaboration of government sectors, private hospitals, and institutes like Kathmandu Institute of Child Health Care is the utter need of today. Establishment of KIOCH in building satellite clinics in all seven provinces of the country seems like an expedient endeavour being taken to reach nooks and corners of the country. Doubtless the solution requires developing more medical students, and training existing ones considering the limited human-resource in medicine as mentioned earlier. No child should be deprived of basic right to health because of what his parents earn, and it is the duty of professional experts, philanthropists, and government to make sure infrastructural, medical, and nutritional facilities are parallely balanced.
References:
Guide to Health Insurance and Healthcare System in Denmark. (2020, September 7). Retrieved from https://www.internations.com: https://www.internations.org/go/moving-to-denmark/healthcare?fbclid=IwAR1VLQVTr8RV_9VpPVa3Aez72hNu6KDwFAxXa2FgEwy2-taFZYTqZehdgEI
Oskar G. Jenni, M. a. (2016). Child Health Care in Switzerland. The Journal of Pediatrics, 203-212.
Sumriddetchkajorn, K., Shimazaki, K., Ono, T., Kusaba, T., Sato, K., & Kobayashi, N. (2019, June 1). Universal health coverage and primary care, Thailand. Bulletin of the World Health Organization. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6560367/.
https://data.worldbank.org/indicator/SP.DYN.TFRT.IN?locations=NP





No comments:
Post a Comment